Tuesday on Wallbuilders Live, Dr. Michelle Cretella represented tiny pediatric breakaway group the American College of Pediatricians. She briefly discussed the organization’s position paper on responding to gender identity issues. In doing so, she said something which caught my irony sensor. It also occurred to me, as it repeatedly has in the discussion of gender dysphoria, how difficult it is to avoid taking extreme positions.
Listen to her response to a question from host Rick Green about how much harm gender dysphoria is causing.
I want to address two claims that came up in this segment. In this post, I address the claim that 80% of gender dysphoric children will accept their biological sex with therapy. In a future post, I will write about the claim about suicide rates.
Cretella says:
They’re [advocates for transgender children] cooperating with, at least, mental confusion. You know, initially, we know that there is psychiatric literature that shows if you work with these children one on one and with their families, the vast majority, over 80% will come to accept their biological sex after puberty before adulthood. So yes, to put these children to reaffirm their confused thinking, to put them on puberty blockers, and then cross-sex hormones to make them quote unquote the other gender, you are permanently sterilizing children. It’s insanity.
Cretella is correct that persistence rates are low (gender dysphoria continuing into adulthood) among gender dysphoric children, but this is not the case with adolescents who remain gender dysphoric or those who experience it with an adolescent onset. In their paper, ACP uses the American Psychiatric Association’s DSM-V as an authority. The section of the DSM-V cited by ACP supports the claim about persistence but does not fully support Cretella’s claim about the role of therapy.
Rates of persistence of gender dysphoria from childhood into adolescence or adulthood vary. In natal males, persistence has ranged from 2.2% to 30%. In natal females, persistence has ranged from 12% to 50%. Persistence of gender dysphoria is modestly correlated with dimensional measures of severity ascertained at the time of a childhood baseline assessment. In one sample of natal males, lower socioeconomic background was also modestly correlated with persistence. It is unclear if particular therapeutic approaches to gender dysphoria in children are related to rates of long-term persistence. Extant follow-up samples consisted of children receiving no formal therapeutic intervention or receiving therapeutic interventions of various types, ranging from active efforts to reduce gender dysphoria to a more neutral, “watchful waiting” approach. It is unclear if children “encouraged” or supported to live socially in the desired gender will show higher rates of persistence, since such children have not yet been followed longitudinally in a systematic manner. For both natal male and female children showing persistence, almost all are sexually attracted to individuals of their natal sex. For natal male children whose gender dysphoria does not persist, the majority are androphilic (sexually attracted to males) and often self-identify as gay or homosexual (ranging from 63% to 100%). In natal female children whose gender dysphoria does not persist, the percentage who are gynephilic (sexually attracted to females) and self-identify as lesbian is lower (ranging from 32% to 50%). (APA, DSM-V, p. 455)
To the DSM-V, I can add the description of persistence developed by the World Professional Association for Transgender Health (WPATH) in their standards of care.
An important difference between gender dysphoric children and adolescents is in the proportion for whom dysphoria persists into adulthood. Gender dysphoria during childhood does not inevitably continue into adulthood.V Rather, in follow-up studies of prepubertal children (mainly boys) who were referred to clinics for assessment of gender dysphoria, the dysphoria persisted into adulthood for only 6–23% of children (Cohen-Kettenis, 2001; Zucker & Bradley, 1995). Boys in these studies were more likely to identify as gay in adulthood than as transgender (Green, 1987; Money & Russo, 1979; Zucker & Bradley, 1995; Zuger, 1984). Newer studies, also including girls, showed a 12–27% persistence rate of gender dysphoria into adulthood (Drummond, Bradley, Peterson-Badali, & Zucker, 2008; Wallien & Cohen-Kettenis, 2008).
In contrast, the persistence of gender dysphoria into adulthood appears to be much higher for adolescents. No formal prospective studies exist. However, in a follow-up study of 70 adolescents who were diagnosed with gender dysphoria and given puberty-suppressing hormones, all continued with actual sex reassignment, beginning with feminizing/masculinizing hormone therapy (de Vries, Steensma, Doreleijers, & Cohen-Kettenis, 2010).
Another difference between gender dysphoric children and adolescents is in the sex ratios for each age group. In clinically referred, gender dysphoric children under age 12, the male/female ratio ranges from 6:1 to 3:1 (Zucker, 2004). In clinically referred, gender dysphoric adolescents older than age 12, the male/female ratio is close to 1:1 (Cohen-Kettenis & Pfäfflin, 2003). (WPATH, p. 11).
The irony of Cretella’s confidence in psychiatric intervention relates to the expulsion from ACP membership of George Rekers who was infamous for his own personal decline and his discredited treatment approach to what was then called gender identity disorder. In fact, we don’t know the role, if any, therapy plays in influencing the current persistence rates. While there is reason to think parental permission to transition in childhood might increase the persistence rates, there isn’t sufficient research to say for sure.
After listening to Cretella and reading the ACP paper, I wonder what the ACP recommends for the 10-20% of people with gender dysphoria persisting into the late teens. Do they favor reassignment for those persons? They focus on the data which make their point but don’t seem to have an answer for the rest of the people involved.
Another problem with ACP’s confidence in psychiatric interventions for gender dysphoria is that they also oppose a frequent end point in the trajectory of many gender dysphoric children: homosexuality (see image at the end of the post). One of the reasons George Rekers tried to re-orient gender dysphoria was to prevent homosexuality. Furthermore, one of the prime objectives of reparative therapists like Joseph Nicolosi is to prevent homosexuality via the alteration of parenting behaviors toward gender nonconforming children. ACP should stop pretending to sympathize with gender dysphoric children when they also write letters to school personnel promoting reparative change therapy for gay people.
Summary
Cretella is right that studies of gender dysphoric children (mostly with boys) find low rates of persistence of gender dysphoria into adulthood. However, she should have distinguished between prepubescent children and teens. The outcomes for these two groups do not appear to be the same. No doubt her listeners will not make that distinction.
Cretella was wrong to invoke psychiatric treatment as the reason for low persistence rates. If anything, some treatments have been shown to be harmful in some cases while others may not be harmful but may not cause a reduction in gender dysphoria. From her presentation, one could get the impression that advocates for gender dysphoric children know these treatments work but are motivated to undermine the natural family and therefore withhold appropriate medical care. While there is strong disagreement among experts and some advocates might oppose traditional families, it is simply not true that gender dysphoria could be easily treated if only activists would get out of the way.
Another important factor is that the treatment advocated by Cretella and the ACP is an outdated, discredited, psychoanalytically based approach which has not shown success. Even among those in the mainstream who are skeptical of puberty blocking drugs, the treatments advocated by ACP are rejected.
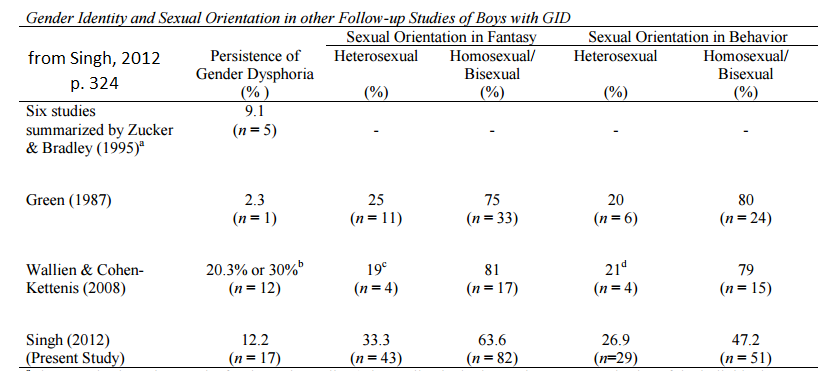
Gender Dysphoria After Childhood
The following image comes from a 2012 study by Devita Singh on gender dysphoric boys. Note the columns titled “sexual orientation in fantasy” and “sexual orientation in behavior.” By far, the most common end point for gender dysphoric children across studies is some level of same sex attraction. Gay advocates have in the past confided to me that they are ambivalent about supporting interruption of puberty because such interventions may interfere with a natural homosexual outcome. Please see this common sense article by Michael Bailey and Eric Vilain on the dilemma many parents of gender dysphoric children face.