Earlier today, the American Psychological Association governing board received the report of the Task Force on Appropriate Therapeutic Response to Sexual Orientation. The report and press release were embargoed until now. With this post, I want to comment on the paper and recommendations made by the Task Force.
Generally, I believe the paper to be a high quality report of the evidence regarding sexual orientation and therapy. The authors of the paper (see this post for the new release which contains authorship information) provide a very helpful discussion of the professional literature on sexual orientation change efforts (SOCE), potential benefits and harm and the role of religion and values in sexual orientation identity exploration. Before I get to a more detailed look at highlights, I want to note an important statement from the APA press release made by Task Force Chair, Judith Glassgold:
Practitioners can assist clients through therapies that do not attempt to change sexual orientation, but rather involve acceptance, support and identity exploration and development without imposing a specific identity outcome.
Dr. Glassgold here describes sexual identity therapy. In fact, as I will point out, the SIT framework is referred to positively throughout the paper. Whereas some evangelicals may be troubled by the negative view of sexual reorientation in this report, there is much here that clarifies important aspects of work in this field. The paper is long (130 pages) and so one post cannot capture all that is important. I want to start with what for me are the high spots, beginning with the abstract:
The American Psychological Association Task Force on Appropriate Therapeutic Responses to Sexual Orientation conducted a systematic review of the peer-reviewed journal literature on sexual orientation change efforts (SOCE) and concluded that efforts to change sexual orientation are unlikely to be successful and involve some risk of harm, contrary to the claims of SOCE practitioners and advocates. Even though the research and clinical literature demonstrate that same-sex sexual and romantic attractions, feelings, and behaviors are normal and positive variations of human sexuality, regardless of sexual orientation identity, the task force concluded that the population that undergoes SOCE tends to have strongly conservative religious views that lead them to seek to change their sexual orientation. Thus, the appropriate application of affirmative therapeutic interventions for those who seek SOCE involves therapist acceptance, support, and understanding of clients and the facilitation of clients’ active coping, social support, and identity exploration and development, without imposing a specific sexual orientation identity outcome. (p. v)
While the paper takes a dim view of change efforts, the authors indicate that attempts to change have been viewed as helpful by some and harmful by others. This is a fair reading of the research. Given these assessments of the research, the stance the APA recommends is to provide supportive psychotherapy without imposing an identity outcome on the client. To get to this view, the authors review change literature, literature on outcomes and research regarding religion and sexual orientation. I want to briefly recap each section.
Efficacy of change efforts
The Task Force reviewed 83 studies that met basic standards for inclusion. They were not impressed with the methodological rigor of the body of research. Their conclusion:
Thus, the results of scientifically valid research indicate that it is unlikely that individuals will be able to reduce same-sex attractions or increase other-sex sexual attractions through SOCE. (p. 3)
Safety of change efforts
The Task Force provided a cautious and nuanced response to the question of harm or benefit from SOCE. I believe they are on target here. Some people report harm and some report benefit but there are no studies which allow conclusions about likelihood of either outcome for any given person. About safety, the press release notes:
As to the issue of possible harm, the task force was unable to reach any conclusion regarding the efficacy or safety of any of the recent studies of SOCE: “There are no methodologically sound studies of recent SOCE that would enable the task force to make a definitive statement about whether or not recent SOCE is safe or harmful and for whom,” according to the report.
Religion and change efforts
One of the highlights of the report is the discussion of religion and sexual orientation. The authors are to be commended for their balanced and thoughtful approach. I especially like the discussion surrounding the concepts of “organismic congruence” and “telic congruence.” On page 18, the paper summarizes these concepts well:
The conflict between psychology and traditional faiths may have its roots in different philosophical viewpoints. Some religions give priority to telic congruence (i.e., living consistently within one’s valuative goals) (W. Hathaway, personal communication, June 30, 2008; cf. Richards & Bergin, 2005). Some authors propose that for adherents of these religions, religious perspectives and values should be integrated into the goals of psychotherapy (Richards & Bergin, 2005; Throckmorton & Yarhouse, 2006). Affirmative and multicultural models of LGB psychology give priority to organismic congruence (i.e., living with a sense of wholeness in one’s experiential self (W. Hathaway, personal communication, June 30, 2008; cf. Gonsiorek, 2004; Malyon, 1982). This perspective gives priority to the unfolding of developmental processes, including self-awareness and personal identity.
This difference in worldviews can impact psychotherapy. For instance, individuals who have strong religious beliefs can experience tensions and conflicts between their ideal self and beliefs and their sexual and affectional needs and desires (Beckstead & Morrow, 2004; D. F. Morrow, 2003). The different worldviews would approach psychotherapy for these individuals from dissimilar perspectives: The telic strategy would prioritize values (Rosik, 2003; Yarhouse & Burkett, 2002), whereas the organismic approach would give priority to the development of self-awareness and identity (Beckstead & Israel, 2007; Gonsiorek, 2004; Haldeman, 2004). It is important to note that the organismic worldview can be congruent with and respectful of religion (Beckstead & Israel, 2007; Glassgold, 2008; Gonsiorek, 2004; Haldeman, 2004; Mark, 2008), and the telic worldview can be aware of sexual stigma and respectful of sexual orientation (Throckmorton & Yarhouse, 2006; Tan, 2008; Yarhouse, 2008). Understanding this philosophical difference may improve the dialogue between these two perspectives represented in the literature, as it refocuses the debate not on one group’s perceived rejection of homosexuals or the other group’s perceived minimization of religious viewpoints but on philosophical differences that extend beyond this particular subject matter. However, some of the differences between these philosophical assumptions may be difficult to bridge.
On this blog, we have frequently grappled with these differences. Many such discussions have sides talking past each other because different views of congruence are assumed to be determinative. In this CNN clip about the Task Force, Psychiatrist McCommon and I came to about the same conclusion regarding congruence.
There are different assumptions about what best constitutes the answer to the question: ‘who am I?’ This paper nicely addresses these assumptions and acknowledges that people who are deeply committed to a non-gay-affirming religious position may stay same-sex attracted but not identify as gay. As the paper notes, this is an acceptable alternative.
Clinical approaches
The authors consider the role of therapy and ministries groups as aspects of SOCE. What they say about support groups is interesting.
These effects are similar to those provided by mutual support groups for a range of problems, and the positive benefits reported by participants in SOCE, such as reduction of isolation, alterations in how problems are viewed, and stress reduction, are consistent with the findings of the general mutual support group literature. The research literature indicates that the benefits of SOCE mutual support groups are not unique and can be provided within an affirmative and multiculturally competent framework, which can mitigate the harmful aspects of SOCE by addressing sexual stigma while understanding the importance of religion and social needs. (p. 3)
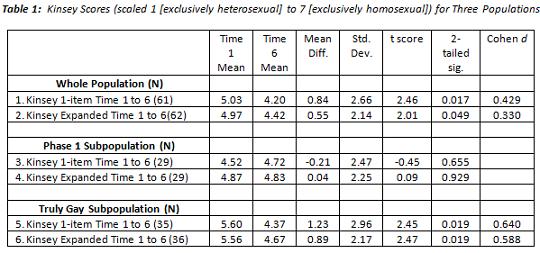
In a nutshell, support groups can have benefit when the singular focus is not change of orientation. Our conversations here regarding the change versus congruence model is relevant. I think the kind of changes that are most common are ideological and behavioral. And when I say behavioral, I mean both cessation of unwanted behavior and also less preoccupation with seeking harmful sexual behavior. I think some people feel they have moved on the Kinsey scale because they have better self-control regarding same-sex behavior. These are good and important telic changes but they don’t represent the kinds of changes which reflect dramatic organismic shifts. Orthodox Christianity does not require organismic changes in order to pursue spiritual development.
Moving from ministry to clinical worlds, the application seems obvious to me. And perhaps it seems obvious since I have been advocating for this stance for several years now. The client sets the value direction and the outcome is not imposed.
In our review of the research and clinical literature, we found that the appropriate application of affirmative therapeutic interventions for adults presenting with a desire to change their sexual orientation has been grounded in a client-centered approach (e.g., Astramovich, 2003; Bartoli & Gillem, 2008; Beckstead & Israel, 2007, Buchanan et al., 2001; Drescher, 1998a; Glassgold; 2008; Gonsiorek; 2004; Haldeman, 2004, Lasser & Gottlieb, 2004; Mark, 2008; Ritter & O’Neill, 1989, 1995; Tan, 2008; Throckmorton & Yarhouse, 2006; Yarhouse & Tan, 2005a; and Yarhouse, 2008). (P.55)
It is heartening to see the SIT framework referenced here (and elsewhere in the APA paper) as one “appropriate application of affirmative therapeutic interventions.” In general, I think the APA strategies and the SIT framework are quite compatible.
Bottom line: The APA report will likely be quite influential for years to come. They call for more research on SOCE and a cautious, and I think accurate, interpretation of the research on reorientation. I believe the therapeutic strategies called for are akin to the SIT framework and clarifies nicely the appropriate stance of therapists. The report also respects the place of religion in identity development and exploration. These issues were not clear prior to this report.
In additional posts, I will deal with various aspects of the paper as well as media coverage. The press release is here and here on the APA website.