I wrote about it when it was news, and now the case has finally been decided. Lesley Pilkington lost.
The article by Strudwick is intriguing and provides insight into the British system — which may be changing if critics have their way.
I wonder who the US conversion therapy organization is…
Category: Professional issues
BYU, Utah professors rebut LDS gay change group
Last Friday, the Salt Lake City Tribune published an opinion article by members of a Latter Day Saint group called Foundation for Attraction Research. This group, co-founded by National Association for the Research and Therapy of Homosexuality leader, Dean Byrd, claims that science validates their religious view of homosexuality. Among other problems, the article last Friday misrepresented the views of National Institute of Health Director Francis Collins.
A week later, today’s SLC Tribune has an effective rebuttal from Wiliam S. Bradshaw, professor emeritus of molecular biology at Brigham Young University; David G. Weight, professor emeritus of clinical and neuropsychology at BYU; and Ted Packard, professor emeritus of educational psychology at the University of Utah. The authors sent the article to me directly:
First, the authors’ manipulations of quotations from Dr. Francis Collins distort and misrepresent his views. They first cite Collins about possible genetic influence on homosexuality. After several intervening paragraphs they introduce separate comments about “individual free will” and “playing the hand dealt to us,” which they represent as his “additional insight on homosexuality.”
This juxtaposition is a deception. The “free will” comments actually refer to genes and intelligence or criminal and antisocial behavior, not homosexuality. Collins has responded to this corruption of his statements by A. Dean Byrd as incoming president of the National Association for Research and Therapy of Homosexuality, or NARTH.
Collins sets the record straight as follows: 1) “The words quoted by NARTH … have been juxtaposed in a way that suggests a somewhat different conclusion than I intended”; 2) The fact that there are other factors that influence how information in DNA is expressed “certainly doesn’t imply that those other factors are inherently alterable”; 3) Even though the actual genes contributing to SSA have yet to be identified, “it is likely that such genes will be found in the next few years.”
Here is the full text of Collins’ unequivocal denunciation of others who, like Byrd and the three authors, have recently misappropriated his scientific views: “It is disturbing for me to see special interest groups distort my scientific observation to make a point against homosexuality. The American College of Pediatricians pulled language out of context from a book I wrote in 2006 to support an ideology that can cause unnecessary anguish and encourage prejudice. The information they present is misleading and incorrect, and it is particularly troubling that they are distributing it in a way that will confuse school children and their parents.”
Regular readers here may recognize the source of this information about Collins – Exgaywatch and then here and here. Read the rest at the link above, I think the authors have made a quality rebutal.
Do gay men have more sexual interest in children than straight men do?
Alice Dreger, writing at the Psychology Today blog, has an important post addressing the title above. Presenting data from Ray Blanchard, she says that the answer to the question is: no, gay men don’t have more sexual interest in children than straight men do. This is an important data set from Blanchard which I am sure will be good news to some and trouble those who want to stigmatize gays.
First a summary from Dr. Dreger:
So, at the outset, let me give away the answer to my headline question: Do gay men have more sexual interest in children than straight men do? No. And we have lab studies to prove it.
In fact, the British Journal of Psychiatry published a major study backing up the “no” answer almost 40 years ago. The distinguished sex researcher Kurt Freund and his colleagues used a laboratory method (described below) that demonstrated that the sexual responses of gay men to boys were similar to the responses of straight men to girls. (Both responses are relatively low.) This past June in Canada, at the major international research conference on sexual orientation science, sex researcher Ray Blanchard (who was trained under Freund) presented substantial new data confirming and expanding on Freund’s findings.
First, Blanchard describes the plethysmograph, which is in essence a means to measure erections in response to various sexual triggers. Although plethysmography has been criticized, it is a direct physical measure which allows comparisons across categories of response. Dreger and Blanchard describe the procedure in detail.
Although the sampling of men in the study raises some concerns, the research is quite relevant to the question about sexual interest. As Dreger notes, the sample is not representative of all men so the numbers of pedophiles are probably inflated compared to the total sample. Given that these are men suspected of a crime or seeking help, one might expect the non-clinical population to test more in keeping with their categorical orientation than this group.
Blanchard’s findings are represented well by this graph:
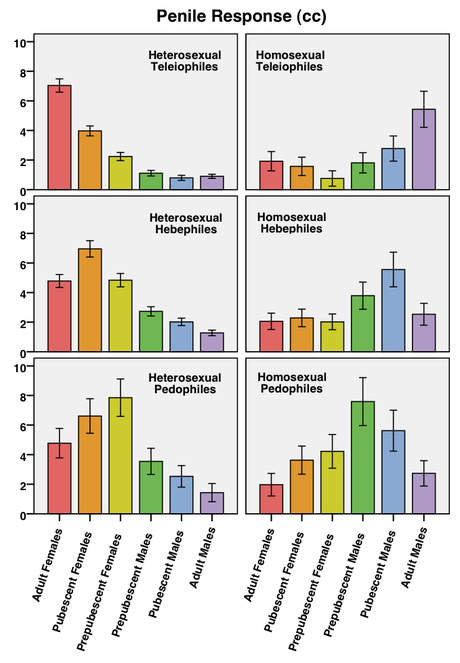
Dreger quotes Blanchard’s explanation for the figure:
This figure shows the mean (average) response of each group to each stimulus category. So that statistically inclined readers can make some comparisons besides those I will explicitly discuss, I have included the 95% confidence interval for each mean. These are represented by the vertical lines bracketing the top of each bar. Two means are significantly different if their confidence intervals do not overlap. The converse, however, is not true, and the significance of the difference between means with overlapping confidence intervals must be tested with methods other than visual inspection.
The key comparisons produced results similar to those of Freund et al. They show that gay men (homosexual teleiophiles) and straight men (heterosexual teleiophiles) have similar penile responses to depictions of children in the laboratory,” that is to say, relatively low. But more important than their being relatively low, they’re not really any different for gay and straight men.
The responses of heterosexual teleiophiles to prepubescent girls were similar to the responses of homosexual teleiophiles to prepubescent boys (gold bar in top left panel vs. green bar in top right panel). The difference between these means was not statistically significant. The responses of heterosexual teleiophiles to pubescent girls were actually slightly higher than the responses of homosexual teleiophiles to pubescent boys (orange bar in top left panel vs. blue bar in top right panel). This difference was statistically significant; however, it is most likely trivial, because the heterosexual teleiophiles were generally a little more responsive than the homosexual teleiophiles.
Dreger concludes: “So it doesn’t look like gay men are any more likely than straight men to be attracted to pubescent children.” Assuming (which seems safe to me) that non-clinical, representative sampling would produce at least the same if not more stable categories, I think Dreger and Blanchard have solid evidence for their conclusion.
Obama Administration rescinds voluntary advance care planning rule
Just about an hour ago, the Health and Human Services Department rescinded the Medicare rule on voluntary advance care planning that had been misrepresented as the return of “death panels” by some social conservatives. I will comment more on this story but for now here is a link to the Federal Register and relevant portions of the order.
II. Provisions of the Amendment
In the July 13, 2010 Federal Register (75 FR 40039), we published the proposed rule entitled “Medicare Program; Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2011.” In response to this publication, we received comments from health care providers, and others urging us to add voluntary advance care planning as a specified element of the definitions of both the “first annual wellness visit” and the “subsequent annual wellness visit.” The commenters stated that their recommendations were based upon a number of recent research studies, and the inclusion by the Medicare initial preventive physical examination (IPPE) provisions of a similar element in the existing IPPE benefit.
CMS agreed with the commenters that voluntary advance care planning should be added as a specified element in the definitions of both the “first annual wellness visit” and the “subsequent annual wellness visit” based on the evidence provided and the inclusion of a similar element in the IPPE benefit (also referred to as the Welcome to Medicare CMS-1503-F2 3 exam) since January 1, 2009, and incorporated it into the final rule.
It has since become apparent that we did not have an opportunity to consider prior to the issuance of the final rule the wide range of views on this subject held by a broad range of stakeholders (including members of Congress and those who were involved with this provision during the debate on the Affordable Care Act). Therefore, we are rescinding the provision of the final rule that includes voluntary advance care planning as a specified element of the annual wellness visits providing personalized prevention plan services, and returning to the policy that was proposed, which was limited to the elements specified in the Act. We are revising our regulation at §410.15(a) to remove voluntary advance care planning as a specified element from the definitions of “first annual wellness visit providing personalized prevention plan services” and “subsequent annual wellness visit providing personalized prevention plan services” and to remove the definition of “voluntary advance care planning.”
And the rule is now amended to read:
For the reasons set forth in the preamble, the Centers for Medicare & Medicaid Services amends 42 CFR part 410 as set forth below:
PART 410–SUPPLEMENTARY MEDICAL INSURANCE (SMI) BENEFITS
1. The authority citation for part 410 continues to read as follows:
Authority (42 U.S.C. 1302, 1395m, 1395hh, and 1395ddd). Secs. 1102, 1834, 1871, and 1893 of the Social Security Act Subpart B–Medical and Other Health Services § 410.15 [Amended]
2. Section 410.15 is amended as follows:
A. In paragraph (a), in the definition of “First annual wellness visit providing personalized prevention plan services” removing paragraph (ix) and redesignating paragraph (x) as paragraph (ix).
B. In paragraph (a), in the definition of “Subsequent annual wellness visit providing personalized prevention plan services” removing paragraph (vii) and redesignating paragraph (viii) as paragraph (vii).
C. In paragraph (a), removing the definition of “voluntary advance care planning”.
Let me note here that in 2008, the same concept was included in the Medicare Improvements for Patients and Providers Act of 2008 and remains a part of Medicare regulations for the first visit by a Medicare enrollee to a physician. George Bush vetoed that bill in 2008 but not because of the end-of-life counseling was included in the bill. He did so because he was concerned that the bill was too costly. I have looked in various search engines for record of opposition to the end-of-life provisions by social conservatives at that time. I found none.
Fact checking the death panel scare
One thing I have learned in the culture wars is to check the specifics of breathless claims from both left and right. So here is a claim from the Liberty Counsel that is making its way around the echo chamber:
Medicare Regulations Revive “Death Panels” of ObamaCare Bill
Is this true? Is Medicare about to unleash a panel of Dr. Deaths on the nation’s elderly? Not at all. This Wall Street Journal article has it about right, describing what Medicare is about to implement via their rule making process:
Advance care planning lays out the options and allows patients, in consultation with their providers and family members, to ensure that their future treatment is consistent with their wishes and moral values should they become too sick to decide for themselves.
To their credit, Liberty Counsel links to the Federal Register issue containing the new regulation, but unfortunately then misrepresents what it says. As noted by the WSJ, discussing advanced directives is something patients should do.
Called “voluntary advance care planning” in the Medicare regulation, this new rule allows physicians to be reimbursed for this consultation during the annual wellness visit, a service allowed by Medicare which covers all sorts of preventive care. The service is defined in the Federal Register:
Voluntary advance care planning means, for purposes of this section, verbal or written information regarding the following areas:
(i) An individual’s ability to prepare an advance directive in the case where an injury or illness causes the individual to be unable to make health care decisions.
(ii) Whether or not the physician is willing to follow the individual’s wishes as expressed in an advance directive. (p. 73406 & 73614).
No death panel there; just the patient, perhaps family, and the physician. Since the conversation is voluntary, a patient can avoid the whole thing. Physicians are allowed to provide written information about how to construct an advanced directive and what individual physicians will do under certain conditions. Physicians must provide informed consent to care and letting patients know what they will do is good practice. If a patient doesn’t like the approach of that doctor, then another doctor can be pursued. I like this approach much better than just waiting around for something to happen and then trying to figure out what the patient would have wanted.
These are important and necessary conversations, even though they can be emotionally difficult. The Federal Register cites studies which suggest that patients appreciate the opportunity to express their wishes and are not harmed by doing so.
Back to the current flap. Where WSJ gets a little misty is when they let Sarah Palin and by extension other fear mongers off the hook a bit by saying that Palin really wants to talk about rationing of care when she writes about “death panels” (as she does here – note the title of the column).
Now I have a whole page on this blog devoted to debunking myths about Sarah Palin so I think it is fair to comment when she is stretching things. If you want to talk about rationing of care, then talk about rationing of care. Voluntarily discussing advanced directives with a personal physician is not a “death panel” nor is it of necessity rationing of care.
Lifenews.com is running a headline claiming that pro-life leaders want the new Congress to overturn the regulation. I am pro-life and I hope the new Congress does not overturn the regulation. I believe physicians should be reimbursed for bringing up the difficult topic and making adequate preparations for the inevitable. Conversations about end-of-life care will happen with or without the regulation. The question is: Will they happen with the patient’s wishes known or not?
UPDATE: Here are some Christian and pro-life groups which advocate advance directives. All the Medicare regulation does is include such planning in annual wellness visits if the patient agrees. Medicare patients could use any of these resources in conversation with their physicians.
Aquinas Institute
Center for Bioethics and Human Dignity
This list was generated after about 5 minutes of searching. I suspect there are other groups with similar recommendations. There is nothing in the Medicare regulations which requires patients to accept a physician’s views if at odds with the patient’s views (although some state laws may allow a physician to ignore advanced directives). Nothing I can find in the Medicare regulation prohibits a patient from drawing on faith based resources to inform these conversations.
Added on Jan 3, 2011: I think it is important to note the voluntary element of these conversations from the Medicare regulations. Advanced care planning may be conducted at the initial Medicare visit and at the annual wellness visit, if the patient agrees. Here is how the Medicare regulation includes the procedure in these visits:
Voluntary advance care planning as that term is defined in this section upon agreement with the individual.