While examining NARTH’s 2009 review of past studies on homosexuality (Journal of Human Sexuality, Vol.1 – click the link for the entire issue), I ran across this citation:
Nicolosi (in press) found that while conducting reparative therapy, a 50-year-old male client reported a sudden and dramatic freedom from unwanted homosexual thoughts, feelings, and behaviors after taking Lexapro. The client reported that he continued to be free of these unwanted symptoms more than 18 months after starting the anti-depressant medicine.
To better examine these claims, I asked one of the authors of the NARTH paper, James Phelan, for access to the source. Thanks to Dr. Phelan for supplying the paper for review.
The paper by Joseph Nicolosi was apparently submitted for publication in 2009 to a journal but there is no record of it being published anywhere. As noted, it describes the case of a 50 year old man who was diagnosed by Nicolosi with ego-dystonic homosexuality. The patient was seen for 142 sessions over “about eight years” with no progress. During therapy, the patient described “generalized hopelessness and helplessness, along with a pervasive sense of inadequacy…” He also described himself as “a non-entity.”
After the lengthy unsuccessful treatment for unwanted same-sex attraction and depression, the patient began taking “a 5 ml dosage of Lexapro,” a selective serotonin reuptake inhibitor. According to Nicolosi, the patient had “an almost immediate decrease in his sense of worthlessness and inadequacy, followed soon after the elimination of his homosexuality.”
The paper describes the situation:
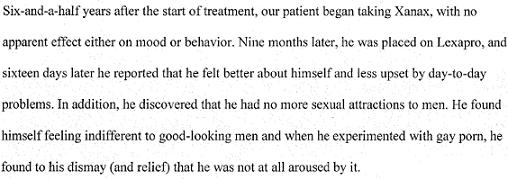
After awhile, the patient stopped taking the drug because he was feeling so much better. However, this brief drug holiday did not work out well.
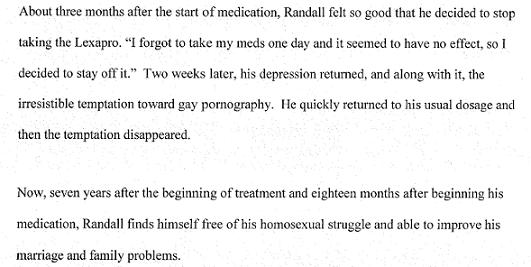
However, there is more to the story.
I wrote to Dr. Nicolosi and asked permission to post the entire paper. He wrote back quickly to clarify that the claim made in the NARTH paper is not longer valid. Nicolosi explained,
I can say that two years later now, that the use of Lexapro has not fulfilled its promise. We no longer see the use of Lexapro as a positive addition to Reparative Therapy.
So another one of the papers referred to in NARTH’s landscape review can be set aside as evidence for sexual reorientation.
Even in Nicolosi’s paper, there was evidence that the medication effect was an anomaly. Nicolosi wrote:
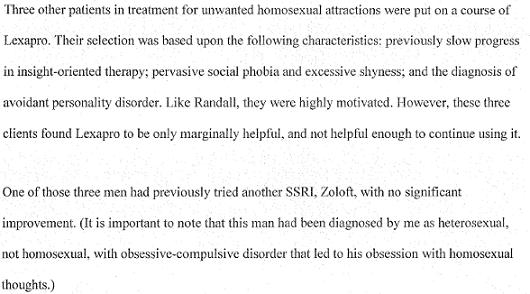
However, these cases were not mentioned in the NARTH review. Instead of noting that the case reported was only one success out of four tries, the authors only noted the one case which appeared to be a success at the time. Now, according to Dr. Nicolosi, Lexapro has not lived up to that claim.
This report can be added to others where significant questions have been raised (e.g., the Bieber study, the Kaye study, the work of Masters and Johnson, the Pattison and Pattison research).
David asked an excellent question:
Wasn’t it Mark Yarhouse who said:
I interact with many “ex-gay/reparative therapy” cast-offs and drop outs every day, and they all express that (years later) they continue to battle feelings of self-loathing, disappointment, resentment and shame because they failed to “change” as promised.
Fortunately, many also find support in coming to terms with their sexual orientation and go on to live productive, balanced and happy lives, intergrating their spirituality and homosexual orientation. I believe that should be the focus of pastoral and professional care — not orientation change.
I imagine that Nicolosi must have become very discouraged that this patient wasn’t showing much progress after 8 years of “insight-oriented” treatment — and finally decided to try something else.
Perhaps he was not aware of the research that shows the effectiveness of a dual-pronged approach to treating depression: a combination of cognitive-behavioral therapy plus anti-depressant medication.
Nicolosli treated this guy for eight years, with all those classic symptoms of depression, before giving him an anti-depressant? It is my understanding that such medications are given early on so that the patient can benefit from the psychotherapy. Eight years sounds like malpractice to me. When you compound it with pseudo-scientific reparative therapy, it almost certainly has to be.
Sometimes, I get the feeling that the folks at NARTH skipped class that day.
It is interesting to me that Nicolosi diagnosis the patient at heterosexual yet the patient is attracted to men and loves gay porn. Does this make sense to anybody? I am not even an armchair psychologist, but it sure seems to me that Randall is gay not heterosexual.
I guess it makes sense to people who believe that no one is really homosexual in orientation — that we are all intrinsically straight — and that gayness is some sort of “block” to one’s innate heterosexuality.
When he describes the other three men he put on Lexapro, when he describes their problems, is Lexapro an appropriate drug for those conditions/problems?
I would venture to guess that’s because you would have provided coherent and scientifically supported treatment plans. Nicolosi would never have passed muster.
If I understand the post here, the article being discussed was never published.
I’m delighted to see this post, since it’s related to a question I brought up a few weeks ago on a different thread — namely, is it possible that some “ex-gay” clients of NARTH or Exodus or whatever are confusing the side effects of anti-depressants (namely, loss of horniness) with the results of the “ex-gay” therapy?
David, Great closing paragraph in your last comment!
While this is off topic, there are big differences between PPO and HMO plans. By definition, PPO plans will not have pre-authorization and heavy reviews. Also, while I can only comment on my clinical practice in Cambridge Massachusetts, and I am aware that I practice in an affluent area in a state with excellent insurance laws, I’ve done over 100 reviews with insurance companies and have been turned down for treatment request authorizations twice. Insurance companies are difficult to deal with, and restrictive, but I find that most don’t understand how insurance works, don’t understand how the law works, and lack the skills to effectively advocate for themselves with insurance companies who are interested in saving money.
JEM, you’re probably correct that my insurance will have changed its rules but I don’t feel the need to go any more.
Furthermore, any provider who submitted a treatment plan with homosexuality as a diagnois would have been promply dropped from the provider panel. We at least required a working knowledge of the DSM.
And this is the problem with NARTH and their shoddy “peer-review” system. Had this been reviewed by professionals, It never would have made it to publication. They would have easily picked up that the efficacy he is describing is likely a result of the common sexual dysfunction associated with most antidepressants, especially of the SSRI class. And (as previously mentioned by the psychologist above), the most commonly reported types of sexual dysfunction effects are decreased libido (arousal and interest) and inorgasmia (inability to orgasm) – the very “efficacy” Nicolosi purports the patient to have experienced. This is is NO WAY related to a change in orientation. The very fact that this was ever reported makes the entirety of NARTH seem laughable as a scientific body.
I’d encourage you to contact your health insurance provider. Mental health parity is the law of the land for most health insurance policies. Among other things, the health care reform act that is law (and many Republicans would like to remove from law) mandates that lifetime maximums are removed from policies and that mental illness must be afforded the same benefits that are provided for physical illness.
Why was Lexapro prescribed for social phobias and excessive shyness? Is it indicated for that?
Also, it seems very odd that the first fellow would claim to experience such dramatic effects after 16 days. I believe that Lexapro takes 4-6 weeks to show its full effects.
Finally – 8 years?! I mean, even the Jones and Yarhouse gang got an average (self-reported) 1-point Kinsey shift after 7. Well, like my favorite Christian, Bryan Fischer, wrote recently, if Barry Bonds can set a record for home runs, then that record becomes “possible” for anyone. Even if the odds are 1 in a million, it is still “possible.” So poor old Randall will just have to suck it up for the few decades he has left and spend his time, money and energy in pursuit of the “possible.” Otherwise Jesus won’t love him.
Jayhuck, I didn’t mean to make multiple posts :0. The website was having issues. Warren took down several of my comments and I’m glad he did. I only intended to comment about this one time. When the comments would not stick to the website I tried again, and again, and again LOL!
Jayhuck, I didn’t mean to make multiple posts :0. The website was having issues. Warren took down several of my comments and I’m glad he did. I only intended to comment about this one time. When the comments would not stick to the website I tried again, and again, and again LOL!
SGM –
Looks like you are taking after me with the multi-posts 🙂
Look for the President of NARTH in this anti gay Political video (trailer). But wait aren’t they only a counseling and research organization (?)
http://manhattandeclaration.org/the-movement/blog/11-11-30/The_Problem_with_Same-Sex_Marriage.aspx
SGM –
Looks like you are taking after me with the multi-posts 🙂
Something is wrong with the website here. I wrote a comment about NARTH being in a Political attack video that NOM is using ,and my comment is not in Moderation it simply disappeared 🙁
Dr. Julie Hamilton President of NARTH
http://www.nomblog.com/16310/?doing_wp_cron
Don’t miss out on reading the lovely comments on the NOM blog. Is this the same woman who said at that conference they just had that NARTH is not anti-gay it is a healthcare and research organization. It would be great for Warren to do an article and show the two videos. I hope somebody gets the DVD and transcribes the part with Dr. Hamilton talks.
More NARTH News. What? Don’t I seem to recall this same woman on video at a NARTH conference saying that NARTH is NOT anti-gay that they are simply a healthcare and research organization? Is that the same woman in this video Dr. Julie Hamilton President of NARTH?
I hope somebody buys the DVD and provides us with a transcript of what Dr. Hamilton says. Good work by Jeremy at http://www.GoodAsYou.org
http://www.nomblog.com/16310/?doing_wp_cron to see the video
The biggest player in the fight to deny Civil Rights for sexual minorities, the National Organization for Marriage, now has NARTH in their lineup. Make sure and read the comments on the NOM blog, here is one-
Just every once in a while it would be so nice to see a comment from Warren- I am Dr. Warrenthrockmorton a college professor of psychology and a draft reviewer of the American Psychological Associations task force on the proper Therapudic Response for Sexual Orientation Change efforts and I am here to tell you that it is rare, for anyone to change their sexual orientation.
It would be nice to see a comment from Warren now like maybe on the NOM blog or something, and then setting the record straight. Hopefully somebody will buy this DVD and tell the rest of us what is on it.
Look for the President of NARTH in this anti gay Political video (trailer). But wait aren’t they only a counseling and research organization (?)
http://manhattandeclaration.org/the-movement/blog/11-11-30/The_Problem_with_Same-Sex_Marriage.aspx
Something is wrong with the website here. I wrote a comment about NARTH being in a Political attack video that NOM is using ,and my comment is not in Moderation it simply disappeared 🙁
Dr. Julie Hamilton President of NARTH
http://www.nomblog.com/16310/?doing_wp_cron
Don’t miss out on reading the lovely comments on the NOM blog. Is this the same woman who said at that conference they just had that NARTH is not anti-gay it is a healthcare and research organization. It would be great for Warren to do an article and show the two videos. I hope somebody gets the DVD and transcribes the part with Dr. Hamilton talks.
More NARTH News. What? Don’t I seem to recall this same woman on video at a NARTH conference saying that NARTH is NOT anti-gay that they are simply a healthcare and research organization? Is that the same woman in this video Dr. Julie Hamilton President of NARTH?
I hope somebody buys the DVD and provides us with a transcript of what Dr. Hamilton says. Good work by Jeremy at http://www.GoodAsYou.org
http://www.nomblog.com/16310/?doing_wp_cron to see the video
The biggest player in the fight to deny Civil Rights for sexual minorities, the National Organization for Marriage, now has NARTH in their lineup. Make sure and read the comments on the NOM blog, here is one-
Just every once in a while it would be so nice to see a comment from Warren- I am Dr. Warrenthrockmorton a college professor of psychology and a draft reviewer of the American Psychological Associations task force on the proper Therapudic Response for Sexual Orientation Change efforts and I am here to tell you that it is rare, for anyone to change their sexual orientation.
It would be nice to see a comment from Warren now like maybe on the NOM blog or something, and then setting the record straight. Hopefully somebody will buy this DVD and tell the rest of us what is on it.
Also — ahem, you didn’t hear this from me — I have an “online acquaintanceship” with a professional gay pr0n director, and he has given me to understand that the “inorgasmia” side effects of anti-depressants are known to him.
In other words, he is quite familiar with the problem of “actors” who are able to maintain photogenic erections for hours, but have frustrating difficulty when asked to produce the, um, “money shot.” (Apparently a lot of male porno stars are on anti-depressants — believe it or not!)
I’m delighted to see this post, since it’s related to a question I brought up a few weeks ago on a different thread — namely, is it possible that some “ex-gay” clients of NARTH or Exodus or whatever are confusing the side effects of anti-depressants (namely, loss of horniness) with the results of the “ex-gay” therapy?
Also — ahem, you didn’t hear this from me — I have an “online acquaintanceship” with a professional gay pr0n director, and he has given me to understand that the “inorgasmia” side effects of anti-depressants are known to him.
In other words, he is quite familiar with the problem of “actors” who are able to maintain photogenic erections for hours, but have frustrating difficulty when asked to produce the, um, “money shot.” (Apparently a lot of male porno stars are on anti-depressants — believe it or not!)
David, Great closing paragraph in your last comment!
JEM, you’re probably correct that my insurance will have changed its rules but I don’t feel the need to go any more.
Why was Lexapro prescribed for social phobias and excessive shyness? Is it indicated for that?
Also, it seems very odd that the first fellow would claim to experience such dramatic effects after 16 days. I believe that Lexapro takes 4-6 weeks to show its full effects.
Finally – 8 years?! I mean, even the Jones and Yarhouse gang got an average (self-reported) 1-point Kinsey shift after 7. Well, like my favorite Christian, Bryan Fischer, wrote recently, if Barry Bonds can set a record for home runs, then that record becomes “possible” for anyone. Even if the odds are 1 in a million, it is still “possible.” So poor old Randall will just have to suck it up for the few decades he has left and spend his time, money and energy in pursuit of the “possible.” Otherwise Jesus won’t love him.
I would venture to guess that’s because you would have provided coherent and scientifically supported treatment plans. Nicolosi would never have passed muster.
If I understand the post here, the article being discussed was never published.
While this is off topic, there are big differences between PPO and HMO plans. By definition, PPO plans will not have pre-authorization and heavy reviews. Also, while I can only comment on my clinical practice in Cambridge Massachusetts, and I am aware that I practice in an affluent area in a state with excellent insurance laws, I’ve done over 100 reviews with insurance companies and have been turned down for treatment request authorizations twice. Insurance companies are difficult to deal with, and restrictive, but I find that most don’t understand how insurance works, don’t understand how the law works, and lack the skills to effectively advocate for themselves with insurance companies who are interested in saving money.
And this is the problem with NARTH and their shoddy “peer-review” system. Had this been reviewed by professionals, It never would have made it to publication. They would have easily picked up that the efficacy he is describing is likely a result of the common sexual dysfunction associated with most antidepressants, especially of the SSRI class. And (as previously mentioned by the psychologist above), the most commonly reported types of sexual dysfunction effects are decreased libido (arousal and interest) and inorgasmia (inability to orgasm) – the very “efficacy” Nicolosi purports the patient to have experienced. This is is NO WAY related to a change in orientation. The very fact that this was ever reported makes the entirety of NARTH seem laughable as a scientific body.
Furthermore, any provider who submitted a treatment plan with homosexuality as a diagnois would have been promply dropped from the provider panel. We at least required a working knowledge of the DSM.
This may be, but in reality these HMO and PPO plans tend to have preauthorization and concurrent review procedures in place. I worked for a managed behavioral health care company for many years.
We rarely authorized more than 12 visits total per year. We would never have authorized treatment of severe depressive symptoms without a medication consultation with a good psychiatrist.
Providers were required to submit treatment plans with clear, measurable goals and proposed interventions. Progress (or the lack of it) was closely monitored. Complicated cases required a doctor-to-doctor review. The kind of treatment Nicolosi describes would have gotten a flat “no”.
Jason Evan Mihalko, Psy.D.=
StraightGrandmother= Jason thank you so much for clearing this up for me. I had no idea, none at all.
I’d encourage you to contact your health insurance provider. Mental health parity is the law of the land for most health insurance policies. Among other things, the health care reform act that is law (and many Republicans would like to remove from law) mandates that lifetime maximums are removed from policies and that mental illness must be afforded the same benefits that are provided for physical illness.
I think that someone else mentioned the confusion of causation and correlation. As someone who takes a veritable cornucopia of medication (I have a SEVERE case of PTSD) nothing has ever made me feel less gay. Of course the fact that I have no interest in feeling less gay might have something to do with it. But I digress.
As far as I know, heterosexual and homosexual are not recognized as a diagnosis by any credible professional society or group, anywhere in the world. I am certain that within the United States, no credible society or group considers or thinks of either of these categories as a diagnosis.
No, no cut off limits. Among other things, I think psychologists don’t spend a lot of time educating the public about what therapy actually is, what it does, and what shapes it takes. If we looked at every psychologist, and every client they worked with, the average number of sessions a client actually comes into therapy is about 6 or 7. This is to say, most people, most of the time, have one specific thing they want to talk about, they come in for a relatively short period of time, and leave feeling like they got some tools to understand and manage their life better.
Over the years, a psychologist will start picking up clients who stay a lot longer. Some people have had significant traumas in their life that take years to work through. Some people have a mental illness that requires regular support and monitoring. Some people use therapy to narrate their live–together with their psychologist they explore the details of their life and look at it in new ways. All of these sorts of people tend to stay in therapy for years — sometimes even decades. It is an important part of their lives that they see as transformative, sustaining, or even something that saves their lives.
So imagine a psychologist in practice — they start out a group of clients and most come in for 6 or 7 sessions. Every few months someone starts that stays longer. After a decade of practice most psychologists have a group of very stable clients who stay for years.
So no, there isn’t a “cut off” for how long therapy is. Sometimes a patient is in an ineffective “non-treatment treatment” where the therapist isn’t helping the patient focus on things that are important. That’s not helpful.
In my own practice, it isn’t unusual for me to see people once a week for years (a handful have worked with me since I was a post-doc, and of those some I think will be with me until I retire). It isn’t uncommon for me to see people twice a week, and there are some types of therapy where it is common to see people three or four times a week for years..
David Hart, I am sincerely sorry for the trauma you experienced. (((hugs)))
I am just going to totally show my ignorance here. The only recollections I recall of a psychiatrist or psychologist is the neurotic Woody Allen who sees his psychiatrist ever single day and Bethenay Frankle’s weekly visits to her psychologist. That is it. I don’t know anything else about it. Stephen based on your response I can see how initially you need to see your doctor a lot but how after a while and you get better it tapers off and you see him/her less frequently, call it maintenance. I dunno 8 years and not making any progress (the patient is still gay) doesn’t the psychologist have some kind of ethical obligation to cut the cord already? Otherwise, from the outside, it seems like the doctor is merely exploiting the patient for financial gain.
Maybe after year number 3…or after year number 4.. or after year number 5… or after year number 6… or after year number 7… or after year number 8… maybe the doctor throws up his hands and admits to the patient that he the doctor is not helping him overcome the issues that brought the patient in to see the doctor and perhaps the patients is better off trying with a different psychologist. Ethically isn’t there some point where a doctor should quit on a patient? Because to not quit on the patient is simply obvious exploitation for financial gain because the patient is not making any progress?
And it appears Nicolosi has more than a few patients like Randall, the other 3 guys he references have been going to him for 6 years.
This may be, but in reality these HMO and PPO plans tend to have preauthorization and concurrent review procedures in place. I worked for a managed behavioral health care company for many years.
We rarely authorized more than 12 visits total per year. We would never have authorized treatment of severe depressive symptoms without a medication consultation with a good psychiatrist.
Providers were required to submit treatment plans with clear, measurable goals and proposed interventions. Progress (or the lack of it) was closely monitored. Complicated cases required a doctor-to-doctor review. The kind of treatment Nicolosi describes would have gotten a flat “no”.
Jason Evan Mihalko, Psy.D.=
StraightGrandmother= Jason thank you so much for clearing this up for me. I had no idea, none at all.
Dear SG.
I’m not a psychiatrist but I have been in analysis. 8 years is not a long time for the classic Freudian style (5 times a week), though that’s hardly used any longer. You’d be surprised at the tens of thousands of men and women who used to try to straighten themselves up that way. Anyone who can afford it now most likely wouldn’t dream of trying. Even behaviorists see a patient over a period of years. What seems peculiar to me is how infrequent these visits must have been. When I first started to see a psychiatrist I saw him twice a week for a year or more. Later it dropped to once. I don’t see how one visit every three or four weeks is going to do much of anything even though it is referred to as ‘treatment’ and ‘… slow progress in insight-oriented therapy’ is cited as if it explains some frustration on the Dr’s part at the recalcitrant nature of the patient’s homo fixation. I’m not surprised going was slow I’m only surprised anyone would call such a diluted course as being in any way therapeutic. However, I was never seen by a clinical psychiatrist and perhaps their approach is radically different from the rest of the profession. But I think it safe to assume that Nicolosi makes a good living
These days the limits of the duration of a patient’s therapy is more often set by who provides insurance. I had a lifetime limit of $5,000 which was reached fairly rapidly and I was only paying $85 for a 50 minute hour, the Manhattan norm.
A couple of things jump out – apart from the general hilarity of the piece.
One, the insistence on pornography as an indicator of a general unwholesomeness; it is written of almost as if it’s a drug. The patient, who seems to be based on Dr Jeckyl and Mr Hyde, is relieved of the curse of being aroused by pornography only to find that when he lays off the magic elixir – oh no! – erections return unbidden. This would seem to me to be a moralistic viewpoint masquerading as some kind of ‘scientific’ indicator.
Two: if Nicolosi had been found to be right he would have proved once and for all that one’s sexual orientation is biological and not a matter of falls from grace (see re pornography above). Here’s a stunner: that Nicolosi should have thought it worth try. Perhaps he should persist? Has he tried aspirin? Or vitamin D?
Shame is, of course, the motor that drives reparative treatment. Shame leaves too many of us vulnerable to snake oil salesmen and self-appointed saviors. The best way to fool other people is always to fool oneself first.
I think that someone else mentioned the confusion of causation and correlation. As someone who takes a veritable cornucopia of medication (I have a SEVERE case of PTSD) nothing has ever made me feel less gay. Of course the fact that I have no interest in feeling less gay might have something to do with it. But I digress.
As far as I know, heterosexual and homosexual are not recognized as a diagnosis by any credible professional society or group, anywhere in the world. I am certain that within the United States, no credible society or group considers or thinks of either of these categories as a diagnosis.
No, no cut off limits. Among other things, I think psychologists don’t spend a lot of time educating the public about what therapy actually is, what it does, and what shapes it takes. If we looked at every psychologist, and every client they worked with, the average number of sessions a client actually comes into therapy is about 6 or 7. This is to say, most people, most of the time, have one specific thing they want to talk about, they come in for a relatively short period of time, and leave feeling like they got some tools to understand and manage their life better.
Over the years, a psychologist will start picking up clients who stay a lot longer. Some people have had significant traumas in their life that take years to work through. Some people have a mental illness that requires regular support and monitoring. Some people use therapy to narrate their live–together with their psychologist they explore the details of their life and look at it in new ways. All of these sorts of people tend to stay in therapy for years — sometimes even decades. It is an important part of their lives that they see as transformative, sustaining, or even something that saves their lives.
So imagine a psychologist in practice — they start out a group of clients and most come in for 6 or 7 sessions. Every few months someone starts that stays longer. After a decade of practice most psychologists have a group of very stable clients who stay for years.
So no, there isn’t a “cut off” for how long therapy is. Sometimes a patient is in an ineffective “non-treatment treatment” where the therapist isn’t helping the patient focus on things that are important. That’s not helpful.
In my own practice, it isn’t unusual for me to see people once a week for years (a handful have worked with me since I was a post-doc, and of those some I think will be with me until I retire). It isn’t uncommon for me to see people twice a week, and there are some types of therapy where it is common to see people three or four times a week for years..
Good comments everybody. I am still hoping that a real psychologist will step up and tell me what the guidelines are for treating patients as I don’t know. Is it standard practice to have a patient see you 3 times a month for 8 years?
David Hart, I am sincerely sorry for the trauma you experienced. (((hugs)))
I am just going to totally show my ignorance here. The only recollections I recall of a psychiatrist or psychologist is the neurotic Woody Allen who sees his psychiatrist ever single day and Bethenay Frankle’s weekly visits to her psychologist. That is it. I don’t know anything else about it. Stephen based on your response I can see how initially you need to see your doctor a lot but how after a while and you get better it tapers off and you see him/her less frequently, call it maintenance. I dunno 8 years and not making any progress (the patient is still gay) doesn’t the psychologist have some kind of ethical obligation to cut the cord already? Otherwise, from the outside, it seems like the doctor is merely exploiting the patient for financial gain.
Maybe after year number 3…or after year number 4.. or after year number 5… or after year number 6… or after year number 7… or after year number 8… maybe the doctor throws up his hands and admits to the patient that he the doctor is not helping him overcome the issues that brought the patient in to see the doctor and perhaps the patients is better off trying with a different psychologist. Ethically isn’t there some point where a doctor should quit on a patient? Because to not quit on the patient is simply obvious exploitation for financial gain because the patient is not making any progress?
And it appears Nicolosi has more than a few patients like Randall, the other 3 guys he references have been going to him for 6 years.
Dear SG.
I’m not a psychiatrist but I have been in analysis. 8 years is not a long time for the classic Freudian style (5 times a week), though that’s hardly used any longer. You’d be surprised at the tens of thousands of men and women who used to try to straighten themselves up that way. Anyone who can afford it now most likely wouldn’t dream of trying. Even behaviorists see a patient over a period of years. What seems peculiar to me is how infrequent these visits must have been. When I first started to see a psychiatrist I saw him twice a week for a year or more. Later it dropped to once. I don’t see how one visit every three or four weeks is going to do much of anything even though it is referred to as ‘treatment’ and ‘… slow progress in insight-oriented therapy’ is cited as if it explains some frustration on the Dr’s part at the recalcitrant nature of the patient’s homo fixation. I’m not surprised going was slow I’m only surprised anyone would call such a diluted course as being in any way therapeutic. However, I was never seen by a clinical psychiatrist and perhaps their approach is radically different from the rest of the profession. But I think it safe to assume that Nicolosi makes a good living
These days the limits of the duration of a patient’s therapy is more often set by who provides insurance. I had a lifetime limit of $5,000 which was reached fairly rapidly and I was only paying $85 for a 50 minute hour, the Manhattan norm.
A couple of things jump out – apart from the general hilarity of the piece.
One, the insistence on pornography as an indicator of a general unwholesomeness; it is written of almost as if it’s a drug. The patient, who seems to be based on Dr Jeckyl and Mr Hyde, is relieved of the curse of being aroused by pornography only to find that when he lays off the magic elixir – oh no! – erections return unbidden. This would seem to me to be a moralistic viewpoint masquerading as some kind of ‘scientific’ indicator.
Two: if Nicolosi had been found to be right he would have proved once and for all that one’s sexual orientation is biological and not a matter of falls from grace (see re pornography above). Here’s a stunner: that Nicolosi should have thought it worth try. Perhaps he should persist? Has he tried aspirin? Or vitamin D?
Shame is, of course, the motor that drives reparative treatment. Shame leaves too many of us vulnerable to snake oil salesmen and self-appointed saviors. The best way to fool other people is always to fool oneself first.
Good comments everybody. I am still hoping that a real psychologist will step up and tell me what the guidelines are for treating patients as I don’t know. Is it standard practice to have a patient see you 3 times a month for 8 years?
David asked an excellent question:
Wasn’t it Mark Yarhouse who said:
I interact with many “ex-gay/reparative therapy” cast-offs and drop outs every day, and they all express that (years later) they continue to battle feelings of self-loathing, disappointment, resentment and shame because they failed to “change” as promised.
Fortunately, many also find support in coming to terms with their sexual orientation and go on to live productive, balanced and happy lives, intergrating their spirituality and homosexual orientation. I believe that should be the focus of pastoral and professional care — not orientation change.
@Lynn David, I may be confused, but from my reading of the excerpted material, it was not Randall, the patient reported to have responded to Lexapro, but rather one of three others who had tried Lexapro had also been on Zoloft.
It’s also important to note that there are (and where) at least a dozen good anti-depressant candidates, many SSRI’s. When one does not work, you are cycled to the next until (hopefully) a good match is found. So even if Randall had been one of those who previously took Zoloft with no significant therapeutic effect, eight years without trying others while experiencing such symptoms seems equally bad.
David Roberts:
Precisely.
Even as Lynn David notes, if he had been on Zoloft, it is reasonable to keep an active referral to a psychiatrist or nurse practitioner. I think 70% of patients respond to the first antidepressant prescribed…low responders should be exposed to other anti-depressants.
Warren,
Did you ask Nicolosi if his depression had returned? The Lexipro may have been effective at resolving this if not the unwanted SSA.
A second question is “How much of his self-loathing is rooted in unrealistic expectations for changing his attractions and his failure to do so?”
I think that someone else mentioned the confusion of causation and correlation. As someone who takes a veritable cornucopia of medication (I have a SEVERE case of PTSD) nothing has ever made me feel less gay. Of course the fact that I have no interest in feeling less gay might have something to do with it. But I digress.
As a consumer I have learned the importance of how to read the results of double blind studies. I would never subscribe to observations like these that have not been subjected to rigorous scientific experimentation protocols.
Warren: This article seems to lack a summary. Given the nature of this information (which is just slightly less arcane than the Talmud) a summary would be helpful.
I imagine that Nicolosi must have become very discouraged that this patient wasn’t showing much progress after 8 years of “insight-oriented” treatment — and finally decided to try something else.
Perhaps he was not aware of the research that shows the effectiveness of a dual-pronged approach to treating depression: a combination of cognitive-behavioral therapy plus anti-depressant medication.
@David Roberts – He was formerly on Zoloft.
@Lynn David, I may be confused, but from my reading of the excerpted material, it was not Randall, the patient reported to have responded to Lexapro, but rather one of three others who had tried Lexapro had also been on Zoloft.
It’s also important to note that there are (and where) at least a dozen good anti-depressant candidates, many SSRI’s. When one does not work, you are cycled to the next until (hopefully) a good match is found. So even if Randall had been one of those who previously took Zoloft with no significant therapeutic effect, eight years without trying others while experiencing such symptoms seems equally bad.
Nicolosli treated this guy for eight years, with all those classic symptoms of depression, before giving him an anti-depressant? It is my understanding that such medications are given early on so that the patient can benefit from the psychotherapy. Eight years sounds like malpractice to me. When you compound it with pseudo-scientific reparative therapy, it almost certainly has to be.
David Roberts:
Precisely.
Even as Lynn David notes, if he had been on Zoloft, it is reasonable to keep an active referral to a psychiatrist or nurse practitioner. I think 70% of patients respond to the first antidepressant prescribed…low responders should be exposed to other anti-depressants.
Warren,
Did you ask Nicolosi if his depression had returned? The Lexipro may have been effective at resolving this if not the unwanted SSA.
A second question is “How much of his self-loathing is rooted in unrealistic expectations for changing his attractions and his failure to do so?”
I guess it makes sense to people who believe that no one is really homosexual in orientation — that we are all intrinsically straight — and that gayness is some sort of “block” to one’s innate heterosexuality.
When he describes the other three men he put on Lexapro, when he describes their problems, is Lexapro an appropriate drug for those conditions/problems?
It is interesting to me that Nicolosi diagnosis the patient at heterosexual yet the patient is attracted to men and loves gay porn. Does this make sense to anybody? I am not even an armchair psychologist, but it sure seems to me that Randall is gay not heterosexual.
Sometimes, I get the feeling that the folks at NARTH skipped class that day.
If I did my calculations right this patient visited Dr. Nicolosi 3 times a month for 8 years? 142 visits at, what do you think a visit costs, $100 (?) that is over $14,000. Figure this patient was spending $300 a month for 8 years. Doesn’t psychology have some kind of a cut off limit, like you should be cured in 12 months or something? Maybe after 12 months you come back once a month. I don’t know, I never went to a psychologist nor paid for one, but is this ethical on the part of the Psychologist? What is the cut off limit as far as for how long you should continue treating a patient? I hope a real psychologist answers my question.
Let’s of course not forget that upwards of 60% of people who take SSRI medication experience unwanted sexual side effects — meaning, lack of interest in sex, or lack of ability to have an orgasm, and so on.
In addition to your current thoughtful analysis of NARTH’s endless pseudoscientific claims, it’s also important to point out what most psychology majors learn their first year of college: correlation does not imply causality.
It’s ludicrous to not consider that less interest in sex while taking an SSRI wasn’t caused by a medication that causes a reduction in sexual feelings.
Of course, much (if not everything) that comes from NARTH is ludicrous.
I think that someone else mentioned the confusion of causation and correlation. As someone who takes a veritable cornucopia of medication (I have a SEVERE case of PTSD) nothing has ever made me feel less gay. Of course the fact that I have no interest in feeling less gay might have something to do with it. But I digress.
As a consumer I have learned the importance of how to read the results of double blind studies. I would never subscribe to observations like these that have not been subjected to rigorous scientific experimentation protocols.
Warren: This article seems to lack a summary. Given the nature of this information (which is just slightly less arcane than the Talmud) a summary would be helpful.
@David Roberts – He was formerly on Zoloft.
If I did my calculations right this patient visited Dr. Nicolosi 3 times a month for 8 years? 142 visits at, what do you think a visit costs, $100 (?) that is over $14,000. Figure this patient was spending $300 a month for 8 years. Doesn’t psychology have some kind of a cut off limit, like you should be cured in 12 months or something? Maybe after 12 months you come back once a month. I don’t know, I never went to a psychologist nor paid for one, but is this ethical on the part of the Psychologist? What is the cut off limit as far as for how long you should continue treating a patient? I hope a real psychologist answers my question.
Let’s of course not forget that upwards of 60% of people who take SSRI medication experience unwanted sexual side effects — meaning, lack of interest in sex, or lack of ability to have an orgasm, and so on.
In addition to your current thoughtful analysis of NARTH’s endless pseudoscientific claims, it’s also important to point out what most psychology majors learn their first year of college: correlation does not imply causality.
It’s ludicrous to not consider that less interest in sex while taking an SSRI wasn’t caused by a medication that causes a reduction in sexual feelings.
Of course, much (if not everything) that comes from NARTH is ludicrous.