The official newsletter of the American Counseling Association is called Counseling Today. Unfortunately, only members can get it online so I cannot provide links to the article I want to discuss. In the April, 2007 issue, a pastoral psychotherapist from DC, Stacy Notaras Murphy published an article titled “Strange Bedfellows: Religion and sexual identity in the counseling office.” I have asked Counseling Today for permission to reprint and will link to a copy of it if I hear a positive response. For now, I will have to include excerpts.
The article purports to be an examination of how people deal with religious identity and sexual identity. From early in the piece:
Most counselors agree that sexual identity is a major aspect of personality development. While more in the field are recognizing that spiritual identity informs personality development as well, the intersection of the two hasn’t received much attention. But the connections may seem more natural when both are considered under the umbrella of multicultural competency.
I certainly agree that training programs outside of religious institutions are rarely helping counselors understand the role of religious identity in integrating a sexual identity. In fact, one of the counselors quoted, Michael Kocet, agreed when he said:
“I would like to see AGLBIC [Association for Gay, Lesbian, Bisexual Issues in Counseling] and ASERVIC [Association for Spritual, Ethical, Religious and Value Issues in Counseling] partnering more on how to integrate their two competency models into effective practice with GLBT clients,” he says. “Right now, I think they’re very much treated separately, most likely unintentionally. I think more research should be done on that; it’s an untapped area within the GLBT community.”
I don’t think it is untapped, but I do think counselors are often confused about how to work ethically and helpfully with clients for whom sexuality and religious faith are important and/or in conflict. The AGLBIC competencies do not mention religion. There is no guidance from that group on how to handle religious conflicts. The ASERVIC competencies on the other hand do provide relevant guidance, especially the following ones:
Competency 5 – The professional counselor can demonstrate sensitivity and acceptance of a variety of religious and/or spiritual expressions in client communication.
Competency 6 – The professional counselor can identify limits of her/his understanding of a client’s religious or spiritual expression, and demonstrate appropriate referral skills and generate possible referral sources.
Competency 7 – The professional counselor can assess the relevance of the religious and/or spiritual domains in the client’s therapeutic issues.
Competency 8 – The professional counselor is sensitive to and receptive of religious and/or spiritual themes in the counseling process as befits the expressed preference of each client.
Competency 9 – The professional counselor uses a clients’ religious and/or spiritual beliefs in the pursuit of the clients’ therapeutic goals as befits the clients’ expressed preference.
Note especially competencies 7-9. Religious beliefs are relevant to clients’ therapeutic goals and should reflect clients’ expressed preference.
Now back to the article and I will cut to the chase. The article conspicuously avoided any mention of religious beliefs that view homosexual behavior in a negative manner. The only alternative presented was to adopt a religious identity that is gay affirming. Note the organization presented to counselors as “Sprituality-based Resources” to such clients:
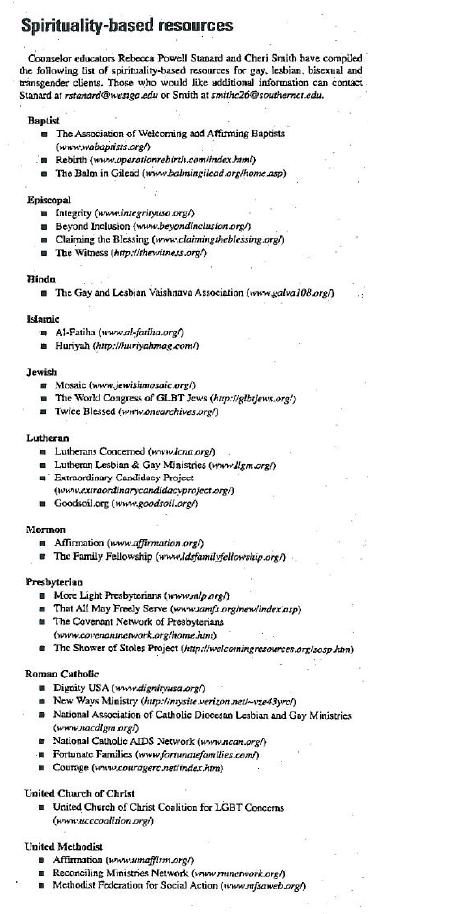
Courage is the only group listed that promotes a traditional sexual ethic. The ASERVIC competency does not call on counselors to endorse or impose a brand of religiousity on clients, rather to use “a clients’ religious and/or spiritual beliefs in the pursuit of the clients’ therapeutic goals as befits the clients’ expressed preference.” What if a client’s expressed preference is for a religious view that is not represented by any group on that list? Then what?
Long time readers will know that the sexual identity therapy framework works within the values and beliefs of the client so I am not advocating for one side here. In fact, what I am saying is that one side will not fit all, even if the exclusion is prefaced by claims of multicultural competence.
UPDATE: I now have permission to post the article. The staff at Counseling Today provided a legible version of the article — thanks to them for that.